Life

Today is the 22nd annual National HIV Testing Day, an event that encourages Americans to learn their HIV status. Thanks to great breakthroughs in treatment, people who find that they are HIV positive have a very different prognosis than they did when the first National HIV Testing Day was observed in 1995. However, it has taken a long time to get to this point, and while it's important to celebrate our progress, it's also important to recognize the struggle that it took to get here.
Human immunodeficiency virus, which was first identified in 1983, has been hugely devastating for many communities across the world. HIV, of course, can potentially develop into AIDS, which lays waste to the immune system, and can lead to death from opportunistic infection. So the stakes of developing effective HIV medication were very high — and tracking the development of treatment is a hair-raising ride.
For many of us, the "AIDS crisis" of the '80s and '90s, when HIV and AIDS were a topic of frequent media coverage, is a distant memory. However, it has remained a serious medical issue ever since it emerged, even if treatments have improved and the CDC has reported a decline in infections; in 2014, there were 1,107,700 adults and teens living with HIV in the U.S., and 6,721 deaths were directly attributed to the disease. And a 2015 HIV crisis in rural Indiana showed that despite all the information that we now have, policy can still create barriers that discourage people from knowing their status, treating their HIV, or taking steps to prevent infection.
So despite what some think, HIV is still an issue, in the US and throughout the world — but it's still key to recognize how far we've come.
1986: The First HIV Drug Offered Little Help Or Hope

The very first HIV drug approved in the US came onto the scene in 1986, and everybody agreed that while it was a breakthrough, it was also deeply imperfect. Zidovudine, or ZDV, was an antiviral that attempted to stop the HIV virus from replicating by blocking an enzyme (its technical name is a "nucleoside analog reverse transcriptase inhibitor"). Other medications in the same class were also rushed onto the market, but they all had pretty serious problems; the Official International AIDS Society Journal notes that they had high toxicity, and that while they seemed to help in the short term, by the time you'd been on them for nearly a year, there wasn't much difference in survival chances. In particular, they were associated with a buildup of lactose in the body, degeneration of the body's fat distribution, and high cholesterol, plus anemia, vomiting and nausea.
Doctors tried to mediate the problem by alternating different types of therapy and adding in new options: ZDV, for instance, was often given with lamivudine, also known as 3TC, another kind of inhibitor; but it still wasn't quite effective enough.
These early days of HIV medication were often filled with a sense of panic, as well as a drive to try and find one big drug that could deal with the entirely of HIV on its own. Called "monotherapy," the approach was relied upon for years. At the same time, the FDA was approving treatments for illnesses specifically related to the decimated immune systems of people with AIDS; in 1988 alone, they approved new drugs to treat pneumonia, Kaposi's sarcoma and retinis in AIDS patients, who often couldn't tolerate standard treatments.
1991: Patients Developed Resistance To Most New Drugs

Scientists kept trying, and from 1991 onwards, they started using another type of inhibitor, called a "non-nucleoside analog reverse transcriptase." It worked in much the same way as ZDV and other drugs, but could be absorbed more quickly. Unfortunately, when it was the only drug being taken, the bodies of HIV patients started to develop resistance to it pretty quickly.
At the same time, scientists developed protease inhibitors, which actively interfere in the "life cycle" of the HIV virus and so try to slow or stop its development. (Interestingly enough, it seems to help with the replication of the hepatitis virus, too).
Alas, first-generation protease inhibitors could only impede the virus for a little while before the infection evolved and the drugs stopped working. The protease inhibitors were also hellish on the liver, and they can't be taken with a lot of other medications because they interfere with how the body processes them. Everything from insomnia to heartburn has been reported as a side effect.
However, a big change was coming: the idea that researchers should be looking for a single miracle drug was becoming less popular — and the age of combined therapy was arriving.
1996: Using Multiple Medicines At Once Offers A Way To Truly Fight The Disease
The biggest moment in the history of HIV and AIDS treatment came in the mid-1990s, just as death tolls from the disease reached unfathomable heights in the US. It was, as experts Michael Shernoff and Raymond A. Williams explained to HIV resource The Body, a product of a new understanding of how HIV worked. Why did all of the earlier drugs stop working after a period of time? Because, they say, the virus was subtly shifting its own genes while replicating, and becoming resistant to drugs:
"... The [HIV] virus gradually becomes less sensitive to specific antiviral medications, a process known as developing resistance. Such resistance generally occurs when a random mutation during the replication of HIV causes a small genetic change in the virus's RNA, in the process making it less vulnerable to the effects of antiviral drugs."
The breakthrough meant scientists now understood why staying on one single medication wasn't helping people with HIV.
And something else happened at the same time: the development of newer, better drugs. An important study reported in 1996 that triple-combination therapy — using ZDV, 3TC and a kind of protease inhibitor — seemed to be massively effective in treatment. The protease inhibitor itself was soon seen to be pretty ineffective and was taken out; but the combination treatment was still a massive jump forward.
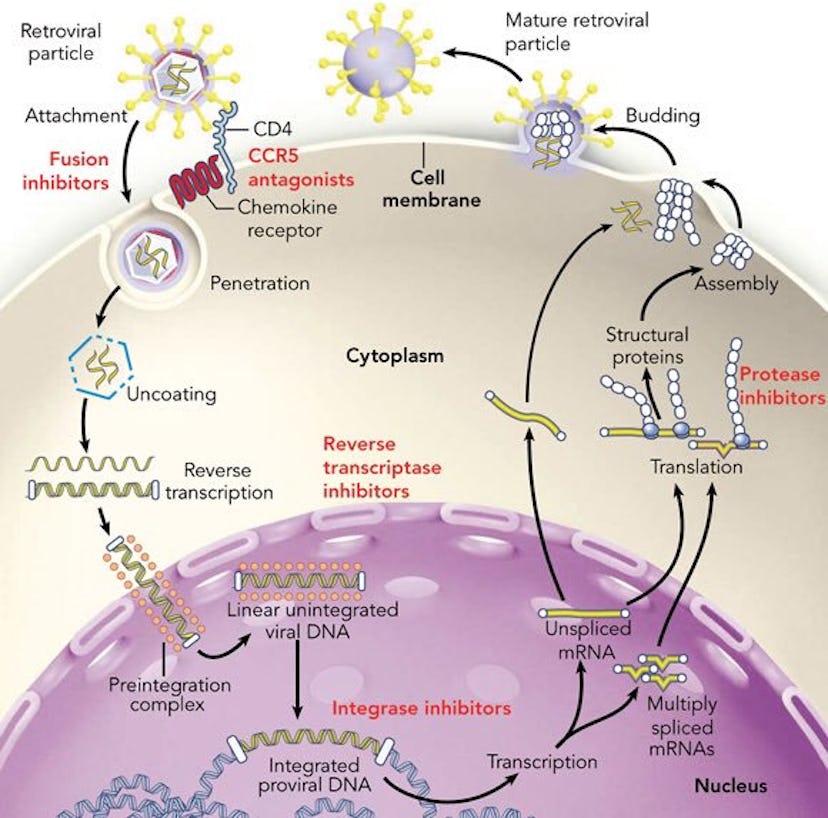
From 1996 onward, it became standard to give HIV patients a "cocktail" of different treatments at once, usually a minimum of three. The variety that could be used in HAART, as it's called (that stands for "highly active antiretroviral therapy"), expanded to include the medication types mentioned above, plus two more: "entry inhibitors", which block HIV's entry into cells, and "integrase inhibitors", which interfere with HIV's genes. This collection of meds led to some seriously good results.
Interestingly, one particular class of HIV treatment has still been investigated as a monotherapy: modern protease inhibitors. While prescribing a combination of drugs to people undergoing HIV treatment is now pretty standard, research conducted in 2016 has shown that just taking this one drug may actually be as good as taking the panoply of others. It's not a solution for all cases, but its an interesting new avenue.
1998: New Testing Changes How Patients Are Monitored & Treated

As the HIV activist group I-Base explains, the breakthrough of combination therapy was based on the discovery of effective testing for levels of HIV in the blood: "Without viral load tests," they say, "combination therapy might never have been developed or understood."
How can you measure whether or not an HIV therapy is actually working? The answer is the viral load test, which takes a milliliter of blood and examines how many virus particles are present in it. This kind of testing is crucial, as the entire point of all the therapies and retroviral medications is to get that level of virus particles as low as possible. Viral load testing developed over the course of the '90s; when it began, it could only detect large viral loads within a blood sample, but by 1998, tests were incredibly sensitive and could test detect small viral loads, too.
Before viral load tests were discovered, scientists thought that HIV had dormant periods, but when the tests emerged in the mid-90s, it became clear that it didn't; even if you weren't currently showing any symptoms, your HIV continued to develop and replicate.
Today: People With HIV Have A Near-Normal Life Expectancy

The advent of HAART has meant big things for people with HIV and their general life expectancy. A new study this past May from the University of Bristol dropped the bombshell that people who've started treatment with today's new, improved HAART cocktails can expect to live nearly as long as people who don't have HIV at all.
Let's put this into context. The World Health Organization estimates that, since it first came onto the scene in the 1980s, 35 million people have died from complications of HIV or AIDS. These days, however, new diagnoses of HIV are falling; between 2005 and 2014, HIV diagnoses fell in the US by 19 percent. This isn't a cure, but it's a huge step forward from an epidemic that has devastated (and in some parts of the world, continues to destroy) huge swathes of the population. Hurrah for the modern world.
The big challenges these days involve getting people tested as early as possible, and getting them the drugs they need. That's where big philanthropic efforts like the Bill & Melinda Gates Foundation are putting their money, but you can do your bit, too. Go have an HIV test, even if you think you're at no risk whatsoever. Knowing the truth never hurts — and in some cases, it can save your life.
